Steroid Source Talk
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
First Cycle
- Thread starter FivePack
- Start date
first cycle you should stick with test cypionate so you don’t have to worry about PIP with test e
Not sure what you mean by that list.
If you’ve never used testosterone before I’d honestly suggest just doing 200-250mg as the weekly dose.
Nothing would be worse then starting out way too high and having no idea what to do when shit hits the fan like getting gyno or not being able to use your dick because your e2 is through the roof
Not sure what you mean by that list.
If you’ve never used testosterone before I’d honestly suggest just doing 200-250mg as the weekly dose.
Nothing would be worse then starting out way too high and having no idea what to do when shit hits the fan like getting gyno or not being able to use your dick because your e2 is through the roof
I literally just learned about PIP Just nowfirst cycle you should stick with test cypionate so you don’t have to worry about PIP with test e
Not sure what you mean by that list.
If you’ve never used testosterone before I’d honestly suggest just doing 200-250mg as the weekly dose.
Nothing would be worse then starting out way too high and having no idea what to do when shit hits the fan like getting gyno or not being able to use your dick because your e2 is through the roof
 . I’m definitely leaning towards a simple cycle of only Testosterone with 200-250mg per week. Can I ask why you suggest Test-C Cypionate as opposed to Test-E Enanthate?
. I’m definitely leaning towards a simple cycle of only Testosterone with 200-250mg per week. Can I ask why you suggest Test-C Cypionate as opposed to Test-E Enanthate?They’re basically the same thing. One has a longer half life by a day or something insignificant like that.I literally just learned about PIP Just now
Test E can be brewed at higher doses. That’s why you usually see Test E at 300mg and Test C at 200 or 250mg
I suggest test c over e as your first cycle becaus UGL test c rarely ever has PIP. Test E you’ll get PIP 9/10 times in UGL and you’ll be limping or have a dead arm and not enjoying your first cycle.
I’ve done test E from a clinic (pharmacy grade) before with zero PIP. Any test e I got UGL always had PIP. Something to do with the test e raws. No one really knows. But there’s no need to deal with that. Just do test c.

Deucalion
Active member
You should get an AI like aromasin or arimidex, HCG if you want to stave off testicular atrophy, Nolvadex in case you run into gyno and you don't want to slam your E2 down, and possibly a bp medication like Telemisartan.
I agree, start at 250 and work your way up so long as you can control sides.I would personally recommend 500mg/ wk max first cycle.
Blood work pre-cycle is HIGHLY recommended. You may run into needing to donate blood if your HGB+HCT get too high on test, I had to my first cycle 3 times...
I agree, start at 250 and work your way up so long as you can control sides.I would personally recommend 500mg/ wk max first cycle.
Blood work pre-cycle is HIGHLY recommended. You may run into needing to donate blood if your HGB+HCT get too high on test, I had to my first cycle 3 times...
Thank you for your response, i’m sure getting an education on pharmaceuticals here. Can you please confirm & clear this up for me. Should one only take an AI if they experience symptoms or as a preventative?You should get an AI like aromasin or arimidex, HCG if you want to stave off testicular atrophy, Nolvadex in case you run into gyno and you don't want to slam your E2 down, and possibly a bp medication like Telemisartan.
I agree, start at 250 and work your way up so long as you can control sides.I would personally recommend 500mg/ wk max first cycle.
Blood work pre-cycle is HIGHLY recommended. You may run into needing to donate blood if your HGB+HCT get too high on test, I had to my first cycle 3 times...
Aromitase Inhibitors - AI
Aromasin - (Exemestane)
Arimidex - (Anastrozole)
Nolvadex - (Tamoxifen)
All three of these drugs lower Estrogen & prevent Gyno - Gynecomastia
HCG - Human Chorionic Gonadotropin
Prevents testicular atrophy
I currently get my blood work done every 3 months for my TRT & I’ve had to blood-let once already so I am familiar with the symptoms now & a blood pressure medication like Telemisartan should not be necessary for me.
There really is a lot more to all of this than one would think. You need to be a scientist/doctor. Now i understand why these products are not easy to get ahold of.
Deucalion
Active member
So, here is the thing. You need nolvadex separate from a real AI in MY OPINION, and this is why. Nolvadex binds to estrogen receptors which blocks estrogen in your blood from binding and exerting an estrogenic effect(mostly). Whereas an AI like arimidex inhibits aromatase from converting T to E1,E2 or E something else lol, I forget that last estrogen it blocks from being created.Thank you for your response, i’m sure getting an education on pharmaceuticals here. Can you please confirm & clear this up for me. Should one only take an AI if they experience symptoms or as a preventative?
Aromitase Inhibitors - AI
Aromasin - (Exemestane)
Arimidex - (Anastrozole)
Nolvadex - (Tamoxifen)
All three of these drugs lower Estrogen & prevent Gyno - Gynecomastia
HCG - Human Chorionic Gonadotropin
Prevents testicular atrophy
I currently get my blood work done every 3 months for my TRT & I’ve had to blood-let once already so I am familiar with the symptoms now & a blood pressure medication like Telemisartan should not be necessary for me.
There really is a lot more to all of this than one would think. You need to be a scientist/doctor. Now i understand why these products are not easy to get ahold of.
Here is the thing lets say you have an E2 of 90 and are having gyno effects(Spicy nips are real bro, it happened to me), you do NOT want a heavy dose of AI, it will make you feel like shit when your E2 slams down from 90 to 30, in my experience not to mention the possibility for you to crash E2(WORST mental and physical feeling).... What you want is nolvadex to immediately start blocking the E2 from worsening the gyno, at the mammary receptors and then to SLOWLY take an AI like arimidex in low doses to decrease E2 over a longer period of time..
I hate to force you to spend money on nolvadex because you may never need it, that is a real possibility, but for the price, I used it one time in a blast/ cruise and it was worth it to have on hand for me.
You say that about your BP until you up that T dose to 500 mg and add on HCG then it's all headaches and BP in the 190/110's ER visit from there man... 40$ on amino asylum just to have... Again, may never need, good in my opinion to have on hand, same with nolvadex. Because if you have a problem like BP or Gyno waiting 2 weeks for it to ship etc is not a good option.
That is great that you got blood work and know that feeling of too much HGB+HCT, smarter then me on my first cycle... I was having heart palpitations working out and was so confused, I was thinking electrolyte imbalance but allas it was an insanely high HGB+HCT haha.
Copy all that Duecalion thanks. Now I understand the phrase “having on hand”. I agree, better to spend the money & have on hand. Question, how well does household Aspirin (Acetylsalicylic Acid) work to manage blood pressure on a cycle? I think I would be nervous to go over 250 mg a week after this bit of research.
Deucalion
Active member
Haha aspirin, not at all, it is an antiplatelet agregator. Unless your blood is pudding it won't move your BP, it is good to take though on gear!Copy all that Duecalion thanks. Now I understand the phrase “having on hand”. I agree, better to spend the money & have on hand. Question, how well does household Aspirin (Acetylsalicylic Acid) work to manage blood pressure on a cycle? I think I would be nervous to go over 250 mg a week after this bit of research.
Case-Akilleez
Active member
Copy all that Duecalion thanks. Now I understand the phrase “having on hand”. I agree, better to spend the money & have on hand. Question, how well does household Aspirin (Acetylsalicylic Acid) work to manage blood pressure on a cycle? I think I would be nervous to go over 250 mg a week after this bit of research.
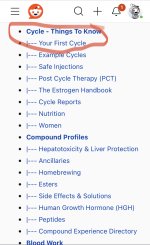
You should consider reading this guide, it will help with a lot of questions you may have, as well as make you consider some things you wouldn’t even know to ask.
There are some things in there I might personally add citations to, or disagree with, but overall it’s a very solid guide. And of course you’re always welcome to continue to ask questions here. There’s many knowledgeable people here who are willing to help and give insight, myself included.
I’d scroll down until you see the section labeled “cycle - things to know”, as shown in this screenshot.
Attachments
Having trouble with the link you sent. Says it’s disabled or doesn’t exist. Is there another way to search for & find the same information?You should consider reading this guide, it will help with a lot of questions you may have, as well as make you consider some things you wouldn’t even know to ask.
There are some things in there I might personally add citations to, or disagree with, but overall it’s a very solid guide. And of course you’re always welcome to continue to ask questions here. There’s many knowledgeable people here who are willing to help and give insight, myself included.
I’d scroll down until you see the section labeled “cycle - things to know”, as shown in this screenshot.
After the past few days of research I’m considering just starting with a short 3-4 week trial of Anavar oral tablets 20-40 mg daily, starting with 10mg then increasing weekly to 20mg, 30mg & finishing with 40mg. Also a PCT of Nolvadex 40mg/day 2 x 20 mg morning/night. Starting with that & seeing what that feels like before diving in head first.
Last edited:
Deucalion
Active member
why would you pct? Unless you plan on coming off TRT too and if that is the case, that sounds like an awful pct...Having trouble with the link you sent. Says it’s disabled or doesn’t exist. Is there another way to search for & find the same information?
After the past few days of research I’m considering just starting with a short 3-4 week trial of Anavar oral tablets 20-40 mg daily, starting with 10mg then increasing weekly to 20mg, 30mg & finishing with 40mg. Also a PCT of Nolvadex 40mg/day 2 x 20 mg morning/night. Starting with that & seeing what that feels like before diving in head first.
Case-Akilleez
Active member
Having trouble with the link you sent. Says it’s disabled or doesn’t exist. Is there another way to search for & find the same information?
After the past few days of research I’m considering just starting with a short 3-4 week trial of Anavar oral tablets 20-40 mg daily, starting with 10mg then increasing weekly to 20mg, 30mg & finishing with 40mg. Also a PCT of Nolvadex 40mg/day 2 x 20 mg morning/night. Starting with that & seeing what that feels like before diving in head first.
Hmm that’s weird. When I click it, it takes me straight to it. You could just go to the website Reddit, type “steroids” in the search bar, and one of the results should be “r/steroids”. Go there and you can find the wiki.
As far as starting with anavar only, you’re free to do as you wish, but I think you’ll be completely underwhelmed. That’s not going to do a whole hell of a lot for you.
I definitely plan on continuing TRT for life. Ok i get it so PCT is only necessary if you’ve added additional Testosterone to the equation?why would you pct? Unless you plan on coming off TRT too and if that is the case, that sounds like an awful pct...
Deucalion
Active member
PCT is POST cycle therapy, it is meant to help you recover your HPTA faster and with fewer sides when you cut the steroids out completely. If you are on TRT you just cruise/blast and manage your E2 sides along the way according to how you feel. It doesn't feel great coming off a 500mg cycle dropping to 150mg(or whatever your TRT dose is) that is why E2 control is important throughout the continuum of your blast/cruise.I definitely plan on continuing TRT for life. Ok i get it so PCT is only necessary if you’ve added additional Testosterone to the equation?
If you are coming off a higher dose of test fast, your E2 should drop equally, the last thing I would want to do is have a moderate E2 to T ratio and then block all E2 effects heavily with nolva. I would still just treat symptoms with AI and serm (nolva). I have never heard of anyone pcting back into a cruise, not in the true PCT sense anyways.
Honestly, pseudoscience here and it could just be me, I wean down my T over about 3 weeks to a TRT dose and plan that into my cycle. It feels better to let your body adjust slowly to T and E2 changes. But because you will be managing E2 sides and not trying to restart your HPTA what is the point of a pct of nolva or any common pct cocktail really?
Deucalion
Active member
Haha exactly! Nolva and arimidex are amazing medications, but you do not want to be on them if you do not need them. Nolva can lower your sex drive and make you feel shitty, not as shitty as a crashed E2 like arimidex can do to you but ya know....Ok that makes sense. I suppose I’m still just realizing that I’m actually getting a solid consistent dose of test from my TRT & that it will always be there so long as I stay on the program.
Deucalion
Active member
I mean that is the gist haha, I have personally never tried aromasin. I have heard people can respond to it much better and for you, it may be better. Arimidex is HARSH at small doses it tanks E2 and it keeps it down for a whileOk so just to summarize
Nolvadex counteracts Gyno
Arimidex controls E2 levels
What is your opinion on Aromasine?
 . 1mg Arimidex which is a big dose can decrease your E2 by 70% in 24 hours, its half-life is 30-60 hours and its full duration is 6 days~. Aromasin I hear is not AS harsh and lasts about half as long as arimidex in the blood. For my cruises, I am going to be looking into aromasin for myself. During a 500 mg blast I have it down pat for arimidex dosing ~1/4th of a .25mg tab 2x a week, my cruising was AWFUL I believe I crashed my E2 3 times and let it rise until I had gyno and was forced to take nolva lol. Wild ride man!
. 1mg Arimidex which is a big dose can decrease your E2 by 70% in 24 hours, its half-life is 30-60 hours and its full duration is 6 days~. Aromasin I hear is not AS harsh and lasts about half as long as arimidex in the blood. For my cruises, I am going to be looking into aromasin for myself. During a 500 mg blast I have it down pat for arimidex dosing ~1/4th of a .25mg tab 2x a week, my cruising was AWFUL I believe I crashed my E2 3 times and let it rise until I had gyno and was forced to take nolva lol. Wild ride man!